



Article
Practice Beat
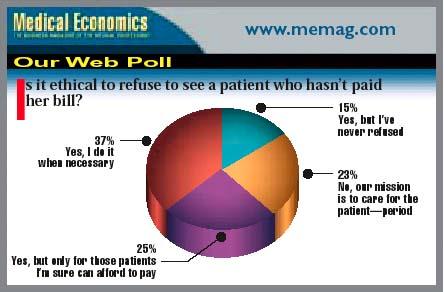
Nurses, Paperwork, Physician Profiles, Hospital Affiliations, Medicare, The Malpractice Crisis, HMOs, Our Web Poll
Practice Beat
Joan R. Rose
Nurses: Job satisfaction: For RNs, a lot depends on you
Obnoxious physiciansand administrators who tolerate themare contributing factors in nurses' decisions to leave their positions, a new VHA study suggests. Overall, 93 percent of the 1,200 nurses, physicians, and hospital executives surveyed had witnessed or experienced disruptive physician behavior, and nearly a third knew at least one nurse who had resigned because of it. Moreover, 24 percent of that group noted that doctors' inappropriate behavior also led nurses to make other changessuch as revising schedules, switching shifts, or changing departmentsto avoid working with those physicians.
Physician Profiles: The push to give patients more information has crossed the border
Manitoba may become the first Canadian province to put physician profiles online. Under legislation proposed by Health Minister Dave Chomiak, The College of Physicians and Surgeons of Manitoba would develop and publicize the profiles, which could include information about a doctor's education, certification, and awards, as well as convictions, disciplinary actions, and malpractice judgments.
The database was recommended after an inquiry into the 1994 deaths of 12 children at Winnipeg's Health Sciences Centre. Many of the parents complained that they weren't given sufficient information about a surgeon to make an informed opinion about whether to use him. They were told that he was "highly trained" and "one of the best," but investigators found that the young surgeon (in his first appointment following residency) lacked the experience and expertise for the job.
Paperwork: One-stop credentialing and formulary searches
The Council for Affordable Quality Healthcare says it has arrived at the Holy Grail of a streamlined, single-application credentialing process and a formulary database, both at no cost to physicians. CAQH's credentialing will permit physicians to submit one applicationeither online or via faxthat will satisfy the requirements of all member health plans and networks, which provide and administer coverage to more than 100 million Americans. The CAQH Formulary DataSource will enable doctors to determine whether a medicine is on a particular health plan's formulary, and, if not, to identify alternatives. (Look for these features at www.caqh.org .)
Hospital Affiliations: Doctors improve hospitals' financial well-being
Most medical specialties, including family practice and internal medicine, generate more than $1 million in net annual revenue for their affiliated hospitals, according to Merritt, Hawkins & Associates, an Irving, TX-based physician recruiting firm. Only three specialtiesophthalmology, otolaryngology, and pediatricsproduce less. Not surprisingly, hospital coffers benefit most from surgical specialties. The high volume of procedures performed by vascular, neurological, and cardiovascular surgeons, for example, bring in $2-3 million annually.


Medicare: CMS wants to revamp the fee schedule, but you'll still lose
The Centers for Medicare & Medicaid Services wants to change how it determines the Medicare physician fee schedule for 2003. CMS' new proposal would modify the methodology used to calculate the Medicare Economic Index (MEI), an inflation measure that is one element of the fee-update formula. The proposed change would, under current estimates, mean that next year's fee payments would drop by an average of 4.4 percent, instead of the 5.1 percent previously projected. But those estimates are expected to be revised later in the year.
To comment on the proposed rule, mail written comments (an original and two copies) to: Centers for Medicare & Medicaid Services, Department of Health and Human Services, Attention: CMS-1204-P, P.O. Box 8013, Baltimore, MD 21244-8013. Comments will be accepted until Aug. 27, and a final Medicare Physician Fee Schedule rule will be published in the fall.
The Malpractice Crisis: Storm clouds form over the Sunshine State
The inability of physicians to purchase affordable liability insurance is one of the most pressing problems Congress needs to deal with, says Rep. Michael Bilirakis (R-FL). The situation is particularly worrisome in his home state where, Bilirakis says, some physicians are paying more than $200,000 a year for coverage.
Now comes news that American Physicians Assurance, an East Lansing, MI-based medical malpractice insurer, is pulling out of the Florida market. Company President/CEO R. Kevin Clinton blames the state's "unpredictable and unfavorable legal climate." The insurer currently writes about 2,200 policies in the state. Although the coverage generated $26.7 million in premiums last year18 percent of the company's totalAPA reported an $18.8 million underwriting loss in Florida.
HMOs: The Supreme Court rules against coverage denials
A closely divided US Supreme Court voted 5-4 to uphold a patient's right to an independent review when an HMO denies approval for a procedure recommended by the patient's physician. The high court's decision, reached in June, upholds an Illinois appellate ruling in a suit brought by Debra Moran against Rush Prudential HMO, now part of Wellpoint. (See "When the HMO says No," May 10, 2002.)
In that case, Moran used the state's patients' rights law to force the HMO to pay $95,000 for complex shoulder surgery after an independent reviewer agreed that the procedure was medically appropriate. Rush claimed the suit was preempted by ERISA, a 1974 federal law that blocks state regulation of managed care plans, and limits plan members' legal options in case of injury.
More than 40 states now have laws that guarantee patients the right to an outside opinion when their health plan turns down a doctor's request for treatment. Similar legislation has been introduced in Congress, but the bills have stalled. Proponents hope this latest Supreme Court ruling will spur Congress to action.


The author is a Contributing Writer.
Joan Rose. Practice Beat. Medical Economics 2002;15:19.










