



Article
Practice Beat
Author(s):
Practice Beat
Practice Beat
By Joan R. Rose, Senior Editor
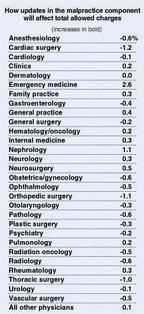
Reimbursement: Medicare continues its transition to resource-based fees
For the first time, Medicare's physician fee schedule in calendar year2000 will reflect a change in the way malpractice costs are calculated.Continuing the payment reforms initiated this year, HCFA will switch froma charge-based formula to one that reflects the actual cost of malpracticeinsurance for each specialty. But don't expect a big boost in fees justbecause your liability coverage is expensive: The change is expected tohave a small-to-negligible effect on physician payments. Of the 30 physiciancategories HCFA uses, 17 will see a decrease, 12 an increase, and one nochange. All changes have to be budget-neutral.
The 2000 fee schedule also reflects further refinement of the way practiceexpenses are estimated. HCFA began a four-year phase-in of resource-basedpractice expenses this year. In 2000, the second year of the phase-in, thatcomponent of physician fees will be based on an equal blend of the charge-basedand resource-based expense RVUs. By 2002, the practice-cost portion of thefee schedule will be fully resource-based. The physician work componentof the fee allowance has been based on RVUs since the introduction of theMedicare fee schedule in 1992; the malpractice component has been basedon historical charges.
Other changes for next year include an increase in the work RVUs forpediatric services, adjustments to the practice-expense RVUs for physicianinterpretation of Pap smears, a reduction in practice-expense payments forclinical office staff time for services performed in a facility setting,and revisions to the work RVUs for new and revised CPT codes for calendaryear 1999.


Source: Federal Register, Nov. 2, 1999
Malpractice: Uncle Sam's attempt to close a data bank loophole fizzles
Under intense pressure from Congress, the Physician Insurers Associationof America, and others, the Health Resources and Services Administrationhas decided to withdraw a proposal that would have changed the reportingrequirements of the National Practitioner Data Bank.
Theoretically, the data bank was created to keep an ongoing record ofphysicians and other practitioners who lose or settle malpractice suits.But some physicians have found a way around that rule by negotiating settlementsin the name of their hospital or practice instead (see Practice Beat, March8, 1999, and Washington Beat, Oct. 25, 1999). HRSA wants to close that loophole.
The agency had proposed that insurers be required to report the nameof any doctor involved in the care of a patient that later became the basisfor a malpractice suiteven if the doctor hadn't been named as a defendant.In addition, payers would have had to include the names of all hospitalsand other entities with which each doctor was affiliated.
The PIAA insists that was the wrong way to go about resolving the problem.Instead of creating new rules, the insurers say it would be more productiveif the NPDB enforced existing laws and regulations. For example, the PIAApointed out, the government's own data suggests that HHS knows the identityof many of those using the "corporate shield" to skirt the law.Yet, the Feds haven't sanctioned or fined any of them. And that failureis the reason underreporting exists, the insurers charge.
Now HRSA Administrator Claude E. Fox says he's "uncomfortable withthe approach set out in the proposed rule,"and he vows to "pullit back and start over."
Baby Numbers
Prenatal care. Last year, 83 percent of mothers-to-be receivedcare during their first trimester. The percentage is the highest ever.
Birth rates. Continuing a seven-year trend, the teen birth ratefell again last yearto 51.1 births per 1,000 women aged 15 to 19. Butthe number of births among unmarried women was about 3 percent higher thanin 1997. Researchers attribute the jump to an increase in the number ofwomen of child-bearing age.
Cesarean deliveries. The number of women having C-sections forthe first time rose 2 percent last yearthe first increase since the federalgovernment began tracking C-sections a decade ago. Overall, cesareans rosefrom 20.8 percent of all births in 1997 to 21.2 percent in '98.
Infant mortality. Although the infant mortality rate last yearmatched the record low set in 1997just 7.2 deaths per 1,000 live birthsitwas the first time in nearly four decades that the rate hadn't improved.And disparities between racial groups also remain, with black infants twiceas likely to die as white infants.
Life expectancy. Children born last year are expected to livefor a record high 76.7 years.
Source: National Center for Health Statistics, "Births and Deaths:Preliminary Data for 1998"
Inpatient Care: California will end the squeeze on nursing services
Over the last several years, hospitals nationwide have cut their nursingstaffs in response to shrinking reimbursement under managed care. Now Californiahas become the first state to enact a law requiring hospitals to meet minimumnurse-to-patient ratios for tasks that come under a nurse's scope of practice.
Under the measure, the state Department of Health Services will determinethe staffing standards for each hospital unitstipulating the various nurseclassifications needed within each unit. Hospitals also will have to adoptwritten policies and procedures for the training and orientation of nursingstaff. As enacted, the law requires DHS to set those minimums by Jan. 1,2001a deadline that likely will be extended by a year.
Claims Review: The ongoing battle of upcoding vs downcoding
This summer, Humana instituted a new nationwide claims-review policythat resulted in widespread downcoding of nearly all level 4 and 5 claimsfor office visits. Now, after meeting with representatives of the Floridaand Texas medical associations, Humana has backtracked.
The HMO says it will no longer review all high-intensity claims.Instead, it will concentrate on those submitted by physicians the plan believesroutinely upcode.
Staff Salaries: Clerical workers are getting much more expensive
Managed care creates greater need for medical office clerical staff,and that demand is beginning to influence their paychecks. Clerical salariesrose an average of 10 percent this year, according to the Professional Associationof Health Care Office Managers. Clinical staff salaries went up only 3 percent.
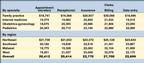
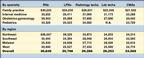
The biggest winners were data entry clerks (who posted a 31 percent gain),followed by billing clerks (25 percent), filing clerks (15 percent), andreceptionists (10 percent). On the clinical side, lab techs earned 11 percentmore this year than last, while RNs saw an increase of 8 percent. Salariesfor LPNs and medical assistants, however, were essentially unchanged from1998.
What selected clerical staffers are earning


What selected clinical staffers are earning


N.A.: not available
Joan Rose. Practice Beat.
Medical Economics
1999;24:27.











